
Background
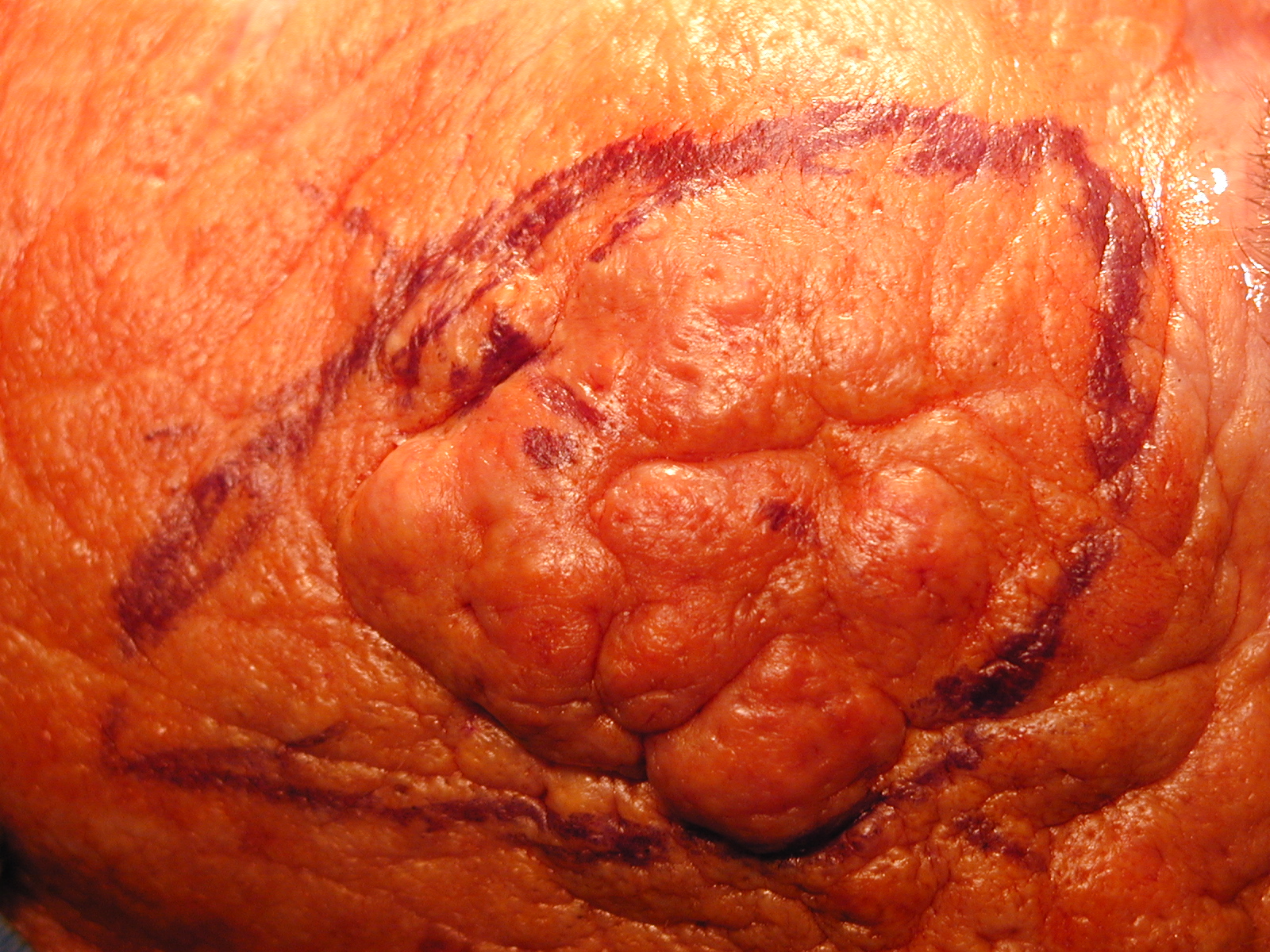
This rare and unusual disease presents with nodules and cysts usually occurring on the cheeks and face of middle aged to elderly patients.
OUTLINE
EPIDEMIOLOGY CHARACTERIZATION SYNONYMS Nodular elastosis with cysts and comedones
DISEASE ASSOCIATIONS CHARACTERIZATION HEMODIALYSIS
Multivariate analysis of cutaneous markers of aging in chronic hemodialyzed patients.Tercedor J, Lopez-Hernandez B, Rodenas JM, Delgado-Rodriguez M, Cerezo S, Serrano-Ortega S.
Department of Dermatology, University of Granada Hospital, Spain.
Int J Dermatol 1995 Aug;34(8):546-50 Abstract quote BACKGROUND: Although hemodialysis has been associated with lesions of cutaneous aging, no controlled studies have been done in patients with chronic renal failure under periodic hemodialysis. Our purpose was to determine the prevalence of several clinical parameters of cutaneous aging and their relationship with hemodialysis.
METHODS: One hundred fourteen patients on chronic hemodialysis were investigated for the presence of several cutaneous aging markers in a cross-sectional study, using multivariate analysis to minimize the confounding effect of age.
RESULTS: Skin cancer was diagnosed in 3 patients (2.6%), actinic keratoses in 12 (10.5%), senile lentigo in 22 (20%), senile purpura in 15 (13%), and Favre-Racouchot disease in 6 (5%). There was no association with skin types or facial wrinkles with any other of the skin-aging features studied. Multivariate analysis, controlling for age as a confounding variable, indicated that the degree of facial wrinkles and the decrease in stratum corneum hydration (capacitance) correlated significantly with the length of time on hemodialysis (P = 0.012 and P = 0.012, respectively). Favre-Racouchot disease (Odds Ratio [OR] = 1.23, P = 0.055, 95% confidence interval [CI] 0.99-1.52) and actinic keratoses (OR = 1.15, P = 0.076, CI 0.98-1.34) became increasingly frequent with the duration of chronic hemodialysis.
CONCLUSIONS: These data show a high prevalence of cutaneous aging lesions in patients on chronic hemodialysis. Acceleration of cutaneous aging is associated with time on hemodialysis.
RADIATION
Favre-Racouchot syndrome associated with radiation therapy.Friedman SJ, Su WP.
Cutis 1983 Mar;31(3):306-10 Abstract quote A 56-year-old woman developed Favre-Racouchot syndrome involving her face and scalp primarily at the sites of x-ray irradiation for therapy of an astrocytoma. The patient had not had comedones prior to radiotherapy and did not have a history of excessive sun exposure.The patient showed an excellent response to topical retinoic acid gel.
To the best of our knowledge, this is the first case of Favre-Racouchot syndrome developing after radiation therapy to be reported in the literature; its pathogenesis is discussed in this paper.
SMOKING Favre-Racouchot syndrome: a case for smokers' comedones.
Keough GC, Laws RA, Elston DM.
Arch Dermatol 1997 Jun;133(6):796-7
GROSS APPEARANCE/
CLINICAL VARIANTSCHARACTERIZATION GENERAL VARIANTS ACTINIC COMEDONAL PLAQUE
Actinic comedonal plaque--a rare ectopic form of the Favre-Racouchot syndrome.John SM, Hamm H.
Department of Health Sciences and Dermatology, University of Osnabruck, Germany.
Clin Exp Dermatol 1993 May;18(3):256-8 Abstract quote A 59-year-old woman with a single cuff-like plaque, consisting of multiple skin-coloured to bluish cysts and comedones on her right forearm is reported.
The solitary lesion resembled, morphologically and histologically, the Favre-Racouchot syndrome. The above condition is another case of the previously described actinic comedonal plaque, which seems to be a rare entity within the spectrum of disease caused by actinic damage to the skin.
UNILATERAL Unilateral nodular elastosis with cysts and comedones (Favre-Racouchot syndrome).
Stefanidou M, Ioannidou D, Tosca A.
Dermatology 2001;202(3):270-1
HISTOLOGICAL TYPES CHARACTERIZATION GENERAL
The histopathology of closed and open comedones of Favre-Racouchot disease.
Sanchez-Yus E, del Rio E, Simon P, Requena L, Vazquez H.
Department of Dermatology, Hospital Universitario San Carlos, Madrid, Spain.
Arch Dermatol 1997 Jun;133(6):743-5 Abstract quote OBJECTIVE: To determine the distinction between a comedo and an infundibular cyst of Favre-Racouchot disease.
SETTING: A university hospital.
PATIENTS: From the 8 patients included in the study, 19 cysts and comedones were evaluated.
MAIN OUTCOME MEASURE: The distinguishing features between the cysts and comedones of Favre-Racouchot disease.
RESULTS: All lesions were histologically indistinguishable from the primary comedones of acne vulgaris, except for the presence of a marked actinic elastosis in the surrounding dermis. The presence of a variable number of hair shafts and an abundant amount of bacteria, which was positive in the results of Gram staining and periodic acid-Schiff reaction and intermingled with sebum and eosinophilic laminated horny material within the dilated infundibulum, characterizes a comedo and differentiates it from an infundibular cyst.
CONCLUSIONS: The cysts and comedones of Favre-Racouchot disease are closed and open comedones. They can be easily differentiated from an infundibular cyst by the histopathologic features rather than by the connection to the surface.
VARIANTS WITHOUT ELASTOSIS
Kerosis and comedos without prominent elastosis in Favre-Racouchot disease.Hassounah A, Pierard GE.
Am J Dermatopathol 1987 Feb;9(1):15-7 Abstract quote Favre-Racouchot disease often is reported to be characterized by the association of cysts and comedos with prominent solar elastosis. Our histological study of patients who rarely exposed themselves to solar irradiation revealed no association between these signs.
We detected only the presence of kerosis, as well as closed and open comedos. There were no true cysts. Actinic damage to the epidermis was absent, and solar elastosis was moderate to discrete.
Therefore, the characteristic follicular alterations in Favre-Racouchot disease appear to be independent of and not secondary to solar elastosis.
DIFFERENTIAL DIAGNOSIS KEY DIFFERENTIATING FEATURES ACNE VULGARIS MYCOSIS FUNGOIDES
Mycosis fungoides and eruptive epidermoid cysts: a unique response of follicular and eccrine structures.Aloi F, Tomasini C, Pippione M.
Department of Dermatology, University of Turin, Italy.
Dermatology 1993;187(4):273-7 Abstract quote A case of a patient who developed simultaneously mycosis fungoides (MF) and multiple, tiny eruptive cutaneous cysts on the face, neck and upper part of the trunk is reported.
Histologically and immunohistochemically MF infiltrate was recognized not only in the upper part of the dermis and in the epidermis but also around and within the walls of cystic lesions. Furthermore, the eccrine structures were also involved by MF infiltrate.
We emphasize that MF infiltrate can affect the follicular and eccrine structures inducing the formation of keratinous cysts. The clinical appearance of the facial lesions may be confused with Favre-Racouchot disease.
PROGNOSIS AND TREATMENT CHARACTERIZATION PROGNOSTIC FACTORS TREATMENT Favre-Racouchot syndrome. A combined therapeutic approach.
Sharkey MJ, Keller RA, Grabski WJ, McCollough ML.
Brooke Army Medical Center, Fort Sam Houston, Tex.
Arch Dermatol 1992 May;128(5):615-6 CURETTAGE Curettage for removal of the comedones and cysts of the Favre-Racouchot syndrome.
Mohs FE, McCall MW, Greenway HT.
Arch Dermatol 1982 May;118(5):365-6 DERMABRASION Dermabrasion for nodular cutaneous elastosis with cysts and comedones. Favre-Racouchot syndrome.
English DT, Martin GC, Reisner JE.
Arch Dermatol 1971 Jul;104(1):92-3 RETINOIDS Treatment of comedos in the Favre-Racouchot disease and acne venenata with vitamin A acid
Hautarzt 1971 Aug;22(8):341-5 Rosai J. Ackerman's Surgical Pathology. Eight Edition. Mosby 1996.
Sternberg S. Diagnostic Surgical Pathology. Third Edition. Lipincott Williams and Wilkins 1999.
Weedon D. Weedon's Skin Pathology. Churchill Livingstone. 1997.
Fitzpatrick's Dermatology in General Medicine. 5th Edition. McGraw-Hill. 1999.
Last Updated 4/30/2002
Send
mail to psdermpath@earthlink.net with
questions or comments about this web site.
Copyright © 2002
The Doctor's Doctor
{kind=link}